
South West Regional Delegation for Public Health in Buea, Cameroon
Strengthening community health workers programmes in conflict settings: Insights from Buea, Cameroon
5 February 2025
Carlson Alinedoh of Queen Margaret University writes on the findings of his study which has looked at strategies to support community health workers (CHWs) working in fragile urban contexts, which has used the anglophone regions in Cameroon as a case study. More on that research here.
“People ask me, ‘Have they given you medicines to come and kill us?’ I have to explain and sometimes take the medicine myself to show it is safe.” For Mola*, a male CHW in Buea, South West Cameroon, such mistrust is a regular occurrence and typical of the challenges faced by CHWs in fragile and conflict-affected settings (FCAS) across the world.
In Buea Health District, an urban and peri-urban setting, CHWs like Mola operate in an environment of protracted conflict and displacement. The Anglophone Crisis [opens new tab], in the north west and south west regions of Cameroon, began in 2016 as a socio-political dispute between the government and English-speaking regions, escalating into an armed conflict. Rooted in historical grievances over marginalisation, the crisis has led to widespread displacement, insecurity, and the collapse of essential services, including healthcare. The persistent insecurity and unstable infrastructure have created barriers to consistent healthcare delivery. In this context, CHWs like Mola have had to navigate these challenges while maintaining their commitment to their communities. However, despite their dedication, CHWs in Buea face numerous obstacles, including threats to their safety, community mistrust, and operational difficulties that make their work increasingly unsafe.
Existing literature and evidence suggests that CHWs are critical to delivering essential health services, particularly in FCAS where formal health infrastructure is often inadequate or disrupted. Given this context, their role has become even more essential as conflict has disrupted conventional healthcare services, making them indispensable in sustaining primary health interventions. As seen in Buea, Cameroon, CHWs act as a vital bridge between communities and health systems, providing preventive, promotive, and curative care despite working in some of the most challenging conditions. Historically, CHWs have struggled with a lack of formal support mechanisms; however, these challenges are significantly exacerbated in FCAS where insecurity, political instability, and resource constraints further strain health service delivery. This study aimed to provide policymakers and health programme designers in western Cameroon with insights into these challenges and to propose context-sensitive strategies to strengthen CHW programmes in FCAS, ensuring their sustainability and effectiveness.

Carl speaks to the CHWs about their challenges and coping mechanisms when working during the conflict
Challenges Faced by CHWs in Buea
Insecurity and physical attacks on CHWS
The ongoing conflict in Buea has placed CHWs at significant personal risk. Many have faced direct threats, abduction, and violence from both armed groups and state actors. As one CHW recounted:
“I lost my child because we couldn’t access a hospital in time… Weeks later, I was abducted and shot by armed groups. Despite everything, I continue my work because the community depends on me.” (Moki, CHW, Buea)
As well as abductions, CHWs have also faced physical attacks from community members who perceive them as government sympathisers due to their involvement in health initiatives. Some have been stoned or harassed while conducting immunisation campaigns.
Mistrust from the community
As the quote at the top of the article shows, CHWs frequently encounter scepticism from the very communities they serve. Given the volatile political landscape, many residents view CHWs with suspicion, associating them with government health initiatives or external interventions. This mistrust is deeply rooted in the historical grievances of the Anglophone regions, where people feel marginalised by the government. The militarised response to the crisis has only exacerbated this suspicion.
This mistrust was most evident during preventive health campaigns, such as immunisation drives, and reached its peak during the COVID-19 pandemic, when misinformation fuelled greater hostility towards CHWs. In contrast, curative services were more readily accepted, as people saw immediate benefits from treatments.
Population Displacement
With thousands displaced due to the conflict, CHWs must often operate in transient and unpredictable environments. The loss of stable community structures complicates outreach efforts, requiring CHWs to adapt to constantly shifting populations.
“At one point, I had to go into the forest to attend to people who had fled there. I took a canoe to reach them, got soaked, but had no choice if I wanted to help.”
(Manga, CHW Buea)
In addition to their communities being displaced, some CHWs themselves have been forced to relocate. This has led to a shortage of CHWs in certain areas, increasing the workload for those who remain.
Coping mechanisms and adaptations
Community support
Despite the challenges, CHWs often find strength in their communities. They rely on informal networks for protection, logistical support, and encouragement.
“The community trusts me because I was chosen by them. They know I work for them, not for the government or any group.” (Eposi, CHW Buea)
While scepticism surrounds certain programmes, many community members continue to value and respect CHWs due to their established relationships and consistent health interventions. This paradox of trust and mistrust reflects the extraordinary circumstances of the crisis, where political and social unrest temporarily disrupt the community’s trust in CHWs.
Operational adaptations
CHWs have developed innovative ways to navigate the dangers of conflict zones, including disguising themselves and adjusting their working hours to avoid detection by armed groups.
“We don’t wear badges anymore. We carry them in our bags and dress casually. In the bush, we put on our gear, do our work, and leave looking like farmers.”
(Manga, CHW Buea)
CHWs also adapted their operations to enhance security. For instance, mosquito nets were stored and distributed at secure locations like former police stations to provide a sense of safety. In other instances, CHWs transitioned from centralised distribution points to door-to-door services to minimise risks. Additionally, to combat misinformation, CHWs used designated forms from the District Health Service to document and relay rumours and false information.
Personal coping strategies
Many CHWs have turned to faith, farming, and alternative livelihoods to manage the stress and economic difficulties of their work.
“When I’m in my farm, I feel connected to life again. It gives me something stable amidst the chaos.” (Moki, CHW Buea)
CHWs’ priorities for support
The study included a participatory ranking exercise in which CHWs were asked to identify and prioritise their support needs. This involved group discussions in which CHWs ranked and justified support strategies based on their perceived relevance and impact.
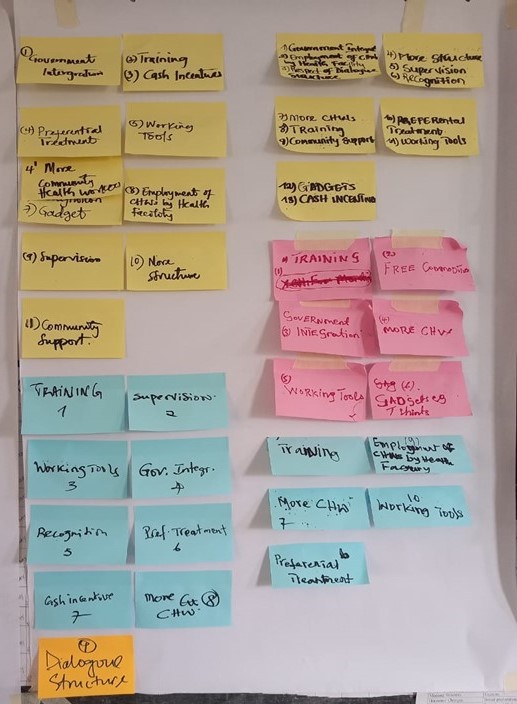
Sample of CHWs’ ranking of preferred support mechanisms in Buea Health District
Compensation and benefits
CHWs overwhelmingly call for regular and fair compensation. Many currently work as volunteers or receive irregular stipends, making it difficult to sustain their families. Providing consistent financial support would improve retention and job satisfaction.
“If the government can’t give us a salary, at least provide the tools to make our work easier.” (Mola, CHW Buea)
Operational support and work environment
CHWs request better equipment, transportation, and protective gear to carry out their duties effectively. Providing these resources would enhance safety and efficiency.
“We need boots, raincoats, and umbrellas. It’s hard to walk miles in bad weather without them.” (Eposi, CHW Buea)
Recognition and status
Many CHWs want formal recognition of their work, including integration into the health system and professional development opportunities. Elevating their status within the health system would validate their contributions and ensure job security.
“We should be acknowledged as professionals. We do more than just help; we save lives.” (Manga, CHW Buea)
An integrated framework for strengthening CHW programmes in FCAS
Based on these findings, one key output from this research was a holistic approach to strengthening CHW programme design in FCAS. This framework proposes considering the interplay between three key elements. First, the CHW programme features, including adequate funding, training for CHWs, structured incentives to motivate their work, and logistical support to ensure they can effectively reach the communities they serve.
The second element is the local context, which encompasses the security risks CHWs may face, the political dynamics at play, cultural perceptions influencing their acceptance, and the availability of resources necessary for program success.
Finally, it is crucial to consider the needs and characteristics of the community health workers themselves. This includes ensuring their safety, providing mental health support to address the stresses of their roles, recognising their professional contributions, and creating pathways for sustainable livelihoods.
By integrating these factors, policymakers and programme designers can develop resilient CHW programmes that remain effective, even in challenging, fragile and conflict-affected environments.
*All names used here are pseudonyms that were changed to protect the identity of the CHWs.